Multi-Center 1002 Patient Clinical Study of Rubimed/Psychosomatic Energetics
Multi-Center 1002 Patient Clinical Study of Rubimed/Psychosomatic Energetics
© 2011 By Dr. Reimar Banis, MND, German
Introduction
Psychosomatic Energetics (PSE) is a relatively new complementary medicine method, developed by Dr. Reimar Banis in the 1990s. Since then, it has been used successfully in many general medicine practices by many specialists, psychotherapists and naturopathic practitioners. Frequently, PSE becomes a key element in these practices and experienced therapists, who have learned and mastered a broad spectrum of therapeutic procedures, often report that they most frequently use PSE. They agree that it quickly "gets to the point", making other procedures unnecessary. As well, many therapists report very good results using PSE in conjunction with psychotherapy, classical homeopathy, Darkfield, or Bach Flower therapy.
At this time, the method is most widely used in German speaking countries and North America. The method is taught on a continuing education basis in multi-day workshops. The entire therapeutic concept is subject to a quality assurance system and is standardized, thus ensuring comparability among therapists. PSE is not ideologically rigid, and specifically recognizes the important role of orthodox medicine. The standard PSE testing procedure can be learned in a weekend seminar, requiring only good energetic testing ability (which experience has shown most therapists do indeed have). Technically and medicinally, PSE is a very manageable and cost-efficient method which can be performed in about 10–15 minutes (with the pre- and post-test discussions taking up most of the time).
As with all new therapeutic methods, the question arises as to how successful it is in daily practice. When a clinical study is done, therapists want an idea of what type of results they will experience in their own practice; they also want more detailed information about diseases and diagnostic groups, i.e. which cases to use the method. In the initial phases of a method, clinical studies serve to gain a preliminary overview of these issues, before undertaking expensive randomized studies later on. To date, two clinical studies have been performed on Psychosomatic Energetics (see Bibliography).
In order to select as broad an initial base as possible, a large multi-centric clinical study began in mid-2006 and concluded in mid-2010. In contrast to the earlier studies, a multi-centric approach was chosen in order to be able to make general statements about PSE. The participants were all professionals who, as "certified energy therapists", had received training in the method and concluded their training successfully. The data was entered online in a predetermined format. The first pass yielded a count of 1504 patients from 14 practices, of which—due to missing classification data, insufficient duration of therapy and other data-input errors—a total of 1002 patients from 11 practices were available to be evaluated. In what follows, I will report on the statistical evaluation and the conclusions from the study. First, however, I'd like to briefly describe the method.
Brief Synopsis of Psychosomatic Energetics (PSE)
The PSE testing sequence is precisely determined, so that test results from different testers can be compared. Using this method, the subtle energy field (the "aural charge") is quantitatively tested. In this process, one determines the percent charge of the vital, emotional, mental and causal energy fields. Sick people usually have very little energy, as do people who feel unwell. In most cases, the energy reading matches the subjective feeling—and often, the clinical finding. Thus, depressive types typically have very low emotional readings, and psychotic types have strikingly low mental readings. When the energy situation is improved by PSE therapy, it often triggers physical and mental self-healing processes. A key component of the method is testing for emotional conflicts using specific homeostatic compound remedies (40 Emvita® "emotional remedies"). Conflicts are considered to be energy thieves as well as subconscious behavior manipulators.
The therapist's examination usually uncovers an active conflict, which the patient, as a rule, agrees is on the mark. For instance, in a burnout patient with an eating disorder, one will find a conflict with the theme of "wanting to have more, frustration". This kind of conflict is considered to be the cause of both the exhaustion and the eating disorder. The tested homeopathic compound remedy is prescribed for a period of months, during which it should permanently dissolve the conflict energetically. After the conflict has been eliminated, most patients report having more energy. This energy increase can be quantitatively verified using the REBA® test device. Moreover, the method has a psychotherapeutic healing effect, thanks to which a patient with an eating disorder can often muster more self-discipline. At the same time, a brief discussion of the conflict theme serves as a "mini-psychotherapy" session which enhances the effectiveness of the prescribed homeopathic compound remedies.
In our experience, more than one conflict needs to be eliminated in over 95% of patients. Since a single conflict dissolution takes 3 to 4 months, a complete PSE course of treatment generally spans a period of 8–15 months. As a rule, positive results can be observed after one or two conflicts have been eliminated. Other therapies can be performed in parallel, such as orthodox medical treatment, psychotherapy or some other naturopathic therapy. However, PSE as a therapy is often applied all by itself. Treatment is considered to be finished when no new conflict turns up in testing and the patient's overall condition has improved accordingly. The patient takes the tested-out compound remedy for the entire duration of therapy in order to dissolve a particular conflict.
Study Design and Implementation

Each of the participating therapists received a codename, so that they could input their data anonymously on the project webpage of the website www.rubimed.com. Only the project head was then allowed access to all the data for evaluation purposes. Patient data input was also encoded (first and last name initials plus birthdate). Besides duration of therapy, the number of consultations was noted until therapy was concluded. A primary diagnosis was requested, i.e. that for which the patient came in for treatment. These diagnoses were also entered in encoded form. In addition, the diagnoses were later placed in broad diagnostic groups. The therapeutic results were "graded" by the therapists on a scale of 1 (excellent) to 6 (insufficient). Incompletely filled out or non-completed therapies were excluded from the study; unfortunately, this applied to about a third of the data sets, and might indicate hectic practice environments, the anonymity inherent in the large number of participants, and the volunteer nature of the study (no remuneration).
Evaluation
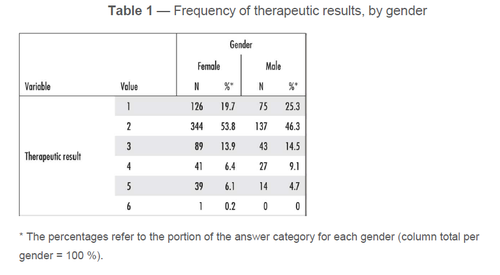
Most of the data came from established general practitioners (81.5%). The average age of the patients was 41.3 years. About two thirds of the patients were female. On average, 4.4 consultations were needed to complete the therapy. Average therapy duration was 15.0 months. In 21.7% of cases the therapeutic result was excellent, in 51% good and in 13.9% satisfactory. Taken together, that yields an overall excellent/good/satisfactory rate of 86.6% of cases. 7.6% of the cases were rated as adequate, 5.8% as deficient, and 0.1% as insufficient. Breakdown by gender shows that these percentages did not differ by all that much; males had more excellent therapeutic outcomes (5.6% more than females), whereas females were somewhat more frequently (7.5% more than men) rated as having good therapeutic outcomes (see Table 1).
After the overall results, there were two questions of interest: 1. What therapeutic results were attained in each diagnostic group? 2. Was there any observable age dependence in the results? As in the earlier general-medicine clinical studies by Dr. Banis and Dr. Holschuh-Lorang, diagnostic groups were created to check whether there were any differences between them, and to see which clinical pictures seemed to respond particularly well to treatment. Concerning the selection of diagnostic groups, I'd like to emphasize that they don't have to do with run-of-the-mill general medicine ailments, but rather above-average difficult and largely therapy-resistant cases. For example, a PSE practice will have a higher than average proportion of patients with chronic pain conditions. In all, seven diagnostic groups were created, corresponding to the frequency of diagnoses and diagnostic groups that one would tend to encounter in a general practice specializing in PSE treatment (see Table 2).
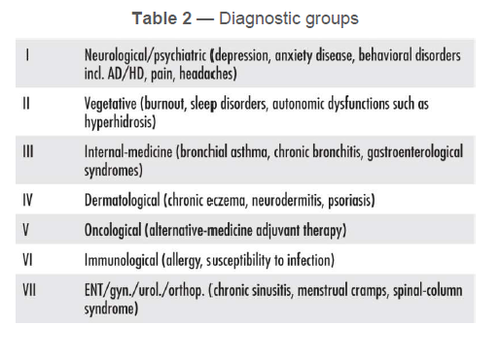
Table 3 summarizes the therapeutic outcomes of all seven diagnostic groups as a bar chart. The differently-colored segments of each bar represent the percentage of patients in a result group for the respective diagnostic group. The result was "graded" using the German school grading system, ranging from 1 (excellent) to 6 (insufficient), which expresses numerically how successful the therapy was thought to be by therapist and patient at the end of therapy. In general, the therapeutic outcomes are relatively uniform in all diagnostic groups. If one defines the categories excellent/good/satisfactory as constituting therapeutic success, then the highest success rates were achieved in group II (vegetative), group III (internal medicine) and group V (oncological). The last-named diagnostic group involves subjective improvement and psychological stabilization; many cancer patients have a geographic stress problem which, when cleaned up, often feels very pleasant and beneficial to most patients. Cancer patients also have higher than average emotional stress, which can also be reduced by PSE. For internal-medicine cases, as well as autonomous vegetative regulatory disorders, emotional problems are known to play a major role, which explains the above-average positive therapeutic outcomes.
Age-Dependency
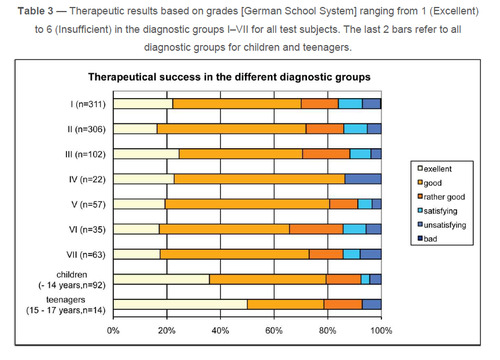
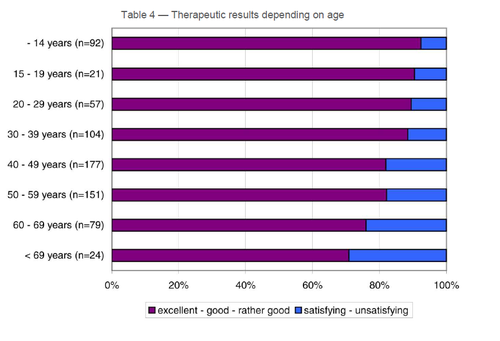
PSE therapy exhibits a clear age dependency (see Table 4). In the group comprised of children and teenagers the rate of excellent therapeutic outcomes is higher than average (see Table 3), amounting to 35.9% for children and 42.9% for teenagers, and dropping to 20% in patients above the age of 50. This is in line with general clinical experience: young people respond more strongly to subtle-energy therapy than do adults.
Comparison with Other Studies
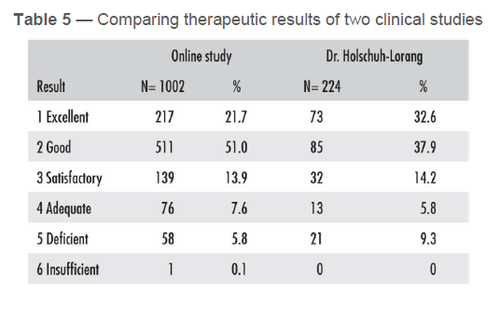
To date, three clinical studies with a total of 1562 patients have been carried out on PSE. Since two of the studies have the same methodological approach and were performed similarly, and moreover shared a therapy duration of 15 months, it clearly makes sense to compare them. Critics are fond of insinuating that alternativemedicine procedures such as PSE only achieve random results. If this were true, one would expect the data to vary widely. Relatively uniform results, on the other hand, substantiate the efficacy of homeopathic and psychosomatic/subtle-energy therapeutic approaches. Table 5 displays the results of both clinical studies with respect to the numeric grades assigned at the end of therapy. Both studies achieved nearly the same excellent and good therapeutic outcomes (72.7% versus 70.5%). If one compares the excellent/good/satisfactory results, they are likewise very similar (86.5% versus 84.8%). In my opinion, this positive comparison validates the idea that PSE is based on principles that, although they can be observed and evaluated empirically in clinical practice, unfortunately cannot yet be understood or explained scientifically.
Summary
The therapeutic success of Psychosomatic Energetics (PSE) was evaluated in a multi-centric clinical study spanning four years. Specially trained therapists from 11 clinical practices took part, with most of them established general practitioners. In all, the data from 1002 patients after 15 months of therapy was evaluated. Every fifth patient had an excellent therapeutic outcome. Over half of the patients reported good results. Combining the excellent, good and satisfactory therapeutic outcomes yields a positive outcome in 86.5% of cases—i.e. the great majority of all patients felt that PSE had been beneficial. When you consider that PSE practices treat predominantly problem patients, the achieved therapeutic outcomes are even more impressive. PSE therapy has shown itself to be a reliable and effective alternative-medicine healing method that can be successfully applied in all current general-medicine clinical pictures. One sees particularly good therapeutic outcomes in children and teenagers, as well as in patients whose clinical picture has a psychosomatic component.
Statistical Evaluation:
Statistician Dr. rer. medic. Silke Lange, Otto-Hue-Str. 19, D-58456 Witten GERMANY
Participating clinics (alphabetically, with patient count in parentheses; for addresses, see therapist directory at www.rubimed.com):
Dr. Reimar Banis and Dr. Ulrike Banis (570), Naturopath Carola Deiss (2), Naturopath Rüdiger Diel (1), Naturopath Ralf Fauser (149), Naturopath Doris Gölz (9), Dentist Dr. Norbert Guggenbichler (4), Dr. Birgitt Holschuh-Lorang (241), Dr. Gabor Littasy (3), Naturopath Sabine Nimphy (10), Dr. Cirsten- Cathrin Thomsen (6).
Bibliography: Banis, R.: Lehrbuch der Psychosomatischen Energetik [Manual of Psychosomatic Energetics] Verlag VAK Kirchzarten 2003 Banis, R. and U. : "Psychosomatische Energetik – Ergebnisse einer Praxisstudie" [Psychosomatic Energet-ics: Results of a Clinical Study], Schweizerische Zeitschrift für Ganzheitsmedizin 3 [Swiss Journal of Ho-listic Medicine], 173-178 (2004) Holschuh-Lorang, B.: "Psychosomatische Energetik in der Allgemeinmedizin – Ergebnisse einer Praxisstudie" [Psychosomatic Energetics in General Medicine: Results of a Clinical Study], Schweizerische Zeitschrift für Ganzheitsmedizin 3 [Swiss Journal of Holistic Medicine], 173-178 (2004)